With the approval of Bill C-218 in June, what will the consequences be for Canadian sports fans?
The unpredictability of sport is attractive.
The sudden turning points at the end of a game entertain the masses and leave them on the edge of their seats. That single unexpected play that turned the game on its head sparks discussion and excitement for hours after the last whistle is blown.
For many, that excitement is usually propelled by external elements. The majority are usually booze-fueled; just intoxicated enough to know what’s going on, but too sloppy to contain themselves with the excitement of a closing play. The minority, however, are fueled by something different: a vice that will now be prevalent in professional sports in North America with the approval of Bill C-218 in June, legalizing single-event sports betting in Canada. That minority might soon become the majority.
Some people find that betting on sports not only provides added excitement, but also keeps those who were once uninterested now glued to the screen. Jack Allen happens to be one of those people. Not being a big sports fan himself, a few single-event side bets on offshore apps like bet365 kept him interested in not only the outcome of the game, but the sport itself.
“[Betting] gave me a reason to actually care about the sport I was watching,” Allen said. “My friends watched sports and I would watch from time to time but wouldn’t really care, but now that betting is involved, I’m more interested in the outcome.”
As of this upcoming season, sports fans will now have the option of betting on multiple factors in one game — the Super Bowl for example — in real time.
According to the Canadian Gaming Association, an estimated 10 billion dollars annually has passed through illegal bookmaking operations. Four billion dollars was spent through offshore betting apps while only 500 million dollars passed through legal provincial lottery processes. In theory, this bill will supposedly eradicate black market gambling, create jobs, and protect consumers, all while establishing a safe and legal betting option.
Entertainment companies have been on the move since the legalization. From Caesars expanding their online betting platform to Ontario, to BetMGM signing Wayne Gretzky in an attempt to expand from coast to coast, one thing is clear: gaming and entertainment companies are competing to become the conglomerate in Canadian sports gambling. However, will repeated exposure and accessibility to sports betting affect people who are most vulnerable? With Ted Leonis, owner of the Washington Capitals in the NHL and Wizards of the NBA granting betting kiosks inside their arena, and more teams to follow suit potentially in the future, where in entertainment do we draw the line?
Dr. John Sader is a family physician who also sub-specializes in addiction. Having worked with all types of patients with varying addictions, Sader believes that not everyone is susceptible to the exposure of gambling in sports.
According to Dr. Sader, addiction depends on factors like inherited genetics, and how those genetics manage dopamine releases in the brain when performing a pleasurable task. From his experience, he explained that on average, 75 per cent of people who suffer from addiction also suffer from a genetic variant of postsynaptic dopamine receptors in the brain.
“There are people who are born with hypo-receptive receptors. With the same level of normal stimulation, they feel much less pleasure.”
In order to feel pleasure, someone who is born with these receptors will ramp up their activity at a higher level than a normal person.
“Addiction has to start somewhere; it starts by liking something too much to the point where you can’t control it anymore,” Dr. Sader said.
The National Council on Problem Gambling released a report before the legalization of single-event betting voicing their concerns over the negative attraction it can have for people, citing that sports betting is twice as likely to occur in comparison to other forms of gambling. With 45 per cent of sports bets conducted online, the rate of exposure and convenience is higher. The report also states that single-event betting offers more betting options on a single game than ever before. The increased speed between bet and reward will also increase the frequency in which people gamble. On top of all this in the age of doing work remotely, people now have more free time on their hands than ever before.
Dr. Sader has personally noticed an uptick in gambling admissions over the course of the pandemic, as people were forced to stay cooped-up inside.
“They can’t go to the restaurant, they can’t go to the movies, they can’t do anything pleasurable. I can only imagine these hypo-dopamine people are suffering even more. Then you start to advertise gambling, and they can do it from their home, it’s on the internet, they start playing and they have fun and a lot of them will get caught up in gambling,” Dr. Sader said.
It’s still too early to tell what effect single-event sports betting will have on sports in general, and the people who watch them. In a time of mass consumption, the approval of this bill will increase viewership and revenue for sports leagues across North America, but at what cost?
As for now, the main challenge for many fans this upcoming season will be toeing the fine line between entertainment and addiction.
Welcome back to your favorite simulation game: University! This fall, as per usual, you can pick and choose which Vice you’d like to play as! There are many options, ranging from extremely serious to relatively innocent coping habits. Remember, each vice comes with some advantages, but mainly downfalls! Take the time to evaluate your life choices this semester – and read these descriptions thoroughly!
The Smoker
This is a timeless vice! Perfect for the fall aesthetic, feed your inner loathing with small “cancer sticks,” as your friends will call them. Of course, smoking cigarettes is bad for you, but it DOES look cool… right? At least, that’s what you thought back when you were 13 picturing what your life would look like now!
Cigarettes are perfect for the procrastinator. These small and inexpensive stinky paper cones will allow you to take excessive breaks all throughout the day, chat with random strangers, and bond over your love of the “forbidden fruit.” According to StatCan, just over 1.5 million Canadians between the ages of 18 and 34 smoke daily or occasionally. When the studying gets going, you’re outside freezing your fingertips off (and trust me, I’m there with you).
The Online Shopper
This one is relatively new! In recent years, going into physical stores has been difficult, not to mention how much work it was to shop in person anyway. Take on a vice that allows you to shop not-so-guilt-free from your couch, bed, or even the bathtub! 94 per cent of Canadians between the ages of 25 to 44 shop online, with average spendings of over $2,000 a year. As students, we already spend so much time online… may as well spend most of your money there. Or, better yet, spend your rent on your fifth matching sweatsuit ‘cause they are just SO comfy.
The one with a JUUL tied to their hand
Yes, this is a different category. This vice, while sharing some of the same components as the cigarette vice (nicotine, the one true addicting queen), is completely different in its application. See, while cigarettes force you to take a break from your hardships, you can vape pretty much anytime, anywhere. This is why it is the perfect vice for those who are just too stressed to take any time off. Let the sweet juice enter your lungs, and set up camp ‘cause the taste of Mango Ice is never leaving the back of your throat.
The Foodie
This vice may seem innocent, but it can wreak havoc on the inside of your bank account. When a university student uses food as a coping mechanism, it will consist mainly of takeout — whether it’s sushi, pizza, tacos, Indian food, or anything else your mouth desires, anything goes! The big problem here is that you lack motivation to cook the giant meal of your dreams, not to mention the work piling up around your takeout containers.
The Drinker
Ah, a classic… Drinking to make it through the school year is the most popular vice. Not only does it help numb you through the endless readings, papers, tests, and lectures, it is also the perfect vice to help you let loose and forget your troubles. This drinking potion is very popular in Canada — a 2016 survey done by the National College Health Assessment survey showed that 35 per cent of students reported having five or more drinks of alcohol per sitting over the last two weeks.
That much alcohol goes against what the Canadian government recommends as a healthy amount, but when have vices been about being healthy? With alcohol, you’ll never be cold, but you might be lonely, since your self-destructive behaviour will push people away faster than you can say “my drink is empty.”
The Stoner
This one is my personal favorite, and one I’ve adopted in everyday life. Weed is one of the most stereotypical “college” things you see — your favourite media tropes of lazy hippie stoners whose eyes won’t open, and are too slow to understand even the simplest joke. This is not my experience, rather that the devil’s lettuce helps to numb me from the realities of my day-to-day life, while still being able to sober up and work (at least a little bit). In terms of how popular weed is, it has seen a rise in recent years with so-called legalization. Back in 2019, just over 50 per cent of Concordia students smoked weed, with 4.2 per cent smoking on a daily basis.
Let’s give an example, shall we? As I write this, I struggle to find the words to describe this lifestyle. I ask myself: ugh why is this so hard to do, as I take my third bowl of the day, and it’s not even 4:20 yet. No wonder I’m having trouble writing.
The resources
On a more realistic note, the point is to highlight the behaviours we tend to adopt during the year, and how these are NOT healthy coping mechanisms. Also, I am guilty of every vice, so this also applies to your humble writer, me. Here are some resources at Concordia University for anyone struggling with mental health issues, drug and alcohol addiction, or anything else. Concordia has a wide variety of mental health support services for you.
Critical masterpiece Brave New World by Aldous Huxley outlines the components of a complicit society — one of pleasure and beauty and a drug called soma. Do we share anything in common?
Have you ever done drugs?
Let me dial back a few notches — what is a drug? Is it a substance that alters a state of consciousness? Something that shimmies around your brain chemistry and makes you feel good?
Are drugs something to be wary of? Like a thief in the night, coming to steal your body’s vitamin C supply, which is a common side effect of smoking?
In these strange times, Aldous Huxley’sBrave New World and its depiction of the drug soma is more relevant and frightening than ever. Our society enjoys drugs in the same way the citizens of the World State do, which is the governing society of Brave New World. This got me thinking: seeing as we are on the brink of complete societal collapse, what is the root function that drugs serve in both of these societies?
Whenever a citizen of the World State has a moment’s pause, or an unpleasant experience, they pop a “gramme” of soma and go on “holiday.” This leaves people with no opportunity or reason to sit and think. It preserves world order.
In present-day North America, we often go on “holiday” like the people of the World State, except in our case, it’s on a screen. We don’t even go number two without zoning out on “holiday” to Netflix, Amazon Prime Video, or Youtube. These days, we don’t think critically about our society’s conventional wisdom and we don’t assess our own thoughts and opinions. Did I think of this idea myself, or did I hear it somewhere? Where did I learn this information? Is this source peer-reviewed? Who conducted this research?
Our soma is literally called Crave, could the message be any clearer? What do you call it when you’re up all night binge watching a show — a bender?
According to the digital Harvard Library, in the 1950s, British neuroscientist John R. Smythies researched the stroboscopic effect on “normal individuals.” According to literary scholar and philosopher Anthony Peake, the stroboscopic effect is when flashing lights create a “flicker effect” in front of the eyes — in other words, what a screen does every time it’s on, whether it be a cellphone, tablet, or computer.
In concluding his research, “Smythies compared the strobe’s “power of addiction” to the powerful drug [mescaline].”
News has become reality television and reality television is now scripted. Thirty-minute Netflix series now end in the middle of the story, and we end up in bed watching marathons instead of running them. Is it all a coincidence?
The hard lines of fact and fiction, of journalism and propaganda, of documentary and reality television, are fading. It’s a dangerous thing that, as more content becomes more accessible, more of our time is spent accessing this content. Commercials are now tied right into the series, as the protagonist breaks the fourth wall and nudges to the audience the shameless product placement.
Is this the holiday soma promised?
I’m left with more questions than answers, but maybe that’s a good thing. It’s important to be critical of our surroundings. How is it that a cellphone plan is now an easy $50 a month? I remember making my first budget when I moved out, and there it was, a $50 cut in my broke-berry pie. When did this become an essential cost of living?
This concept that we need our cellphone is a conventional wisdom of our time. You see the little note taped to your door that reminds you what you need before leaving: “Phone. Keys. Wallet.”
Do I need my phone? Or am I experiencing an addiction to the millions of lights flickering on the screen every time I check it for the time, or get a really well-timed targeted ad.
Isolation has only exacerbated the issue. For those of us fortunate enough to have the option to stay home and self-isolate, most of our communication is taking place on a screen. Hell, I’m writing these words on a screen, and you’re reading it off one. We’re now working from our screens, meeting people from our screens, taking exercise classes from our screens, even having essential services like doctors appointments from our screens.
With all this time spent staring at screens, it would be a good idea to screen the content once in a while. Consider the addictive nature of these devices and take a day off. Since the lights off our phones impact our brains like Mescaline, does that mean you’re getting high right now reading this? Soma promises the people of the World State a holiday, but all my screen promises me is a vitamin C supplement for $29.99, and yours can too if you act now.
‘Addict’ is a label that is often thrown around without much thought. If someone likes something a little too much, they’re considered an addict in the eyes of their entourage.
Addiction is not a quirky way to describe someone’s love and passion for a hobby. The reality is that addiction and negative stereotypes are causing fewer people to seek help, according to Recovery Lighthouse’s website, an addiction recovery clinic. Due to a fear of judgment and rejection, addicts often suffer alone and in silence.
How does addiction start though? An addiction is when people lose control over their consumption behaviours as well as the freedom to stop despite the consequences. Lacking self-esteem or being fueled with high levels of anxiety can exacerbate feelings of loneliness and sadness, due to missing their family and friends.
This loneliness may be the door that lets an addiction makes its way into their life. A person may perceive the consumption of certain substances as helping them cope with their negative feelings. The substance brings instant gratification – a phenomenon where a desire for instant happiness causes the person to do certain acts in order to feel better right away.
Sometimes it’s merely habit-related. Imagine someone drinks every single day at a certain time. The repetition becomes a habit and triggers a need. An addiction will start to form, not only when the person obsessively thinks about drinking, but when habits result in negative consequences. Such consequences can be social isolation from being in a state of enormous exhaustion, caused by the physical and mental toll of over-consumption.
Other symptoms of addiction include depression and high levels of anxiety during periods of withdrawal. Some may become aggressive. Even when the desire is present, cutting back altogether can be difficult when emotions the addiction helped cope with were never really dealt with.
The victim may not be aware of what they’re going through. It is important never to judge a person who is suffering from addiction: you’re never alone.
Picture this: you’re having a crappy day. You missed your bus, spilled coffee down your front and forgot to print out your assignment that’s due in half an hour. To make matters worse, you skipped out on concealer this morning and now look like an extra in Tim Burton’s ‘Corpse Bride.’ (Side note: this scenario may or may not be a projection of my own experiences).
To make yourself feel better, you pop into Simons to buy yourself a new pair of jeans, a sweater and a couple small accessories. By the time the cashier hands you your receipt, the pit of anxiety in your stomach has melted away. You know this purchase is outside your budget, but hey! you’re treating yourself! You’ve had a bad day, after all.
If this sounds familiar to you, you’re not alone. A 2018 survey published by Finder, an online information service for consumers, found that out of 2,000 Canadians, 63 per cent confessed to shopping impulsively in the last year. In the age of mass marketing, online shopping and hyper-consumerism, it’s easier than ever to fall into the trap of impulsive spending. But these impulses go beyond Boxing Day sales and free shipping. According to science, part of the blame can be placed on our biology.
When your brain anticipates a new purchase, it releases a flood of dopamine – that same neurotransmitter associated with drugs, really good food, and really good sex. One study published in Neuron, a neuroscience journal, found that the brain’s reward centre lit up after subjects were shown a desirable product. So, in short, ‘retail therapy’ can serve as a legitimate pick-me-up after a rough day.
But just like food, sex and drugs, shopping can be highly addictive. A study published by the Society for the Study of Addiction gathered data from around the globe and found that shopping addiction affects roughly five per cent of the population. What’s more, research from Cambridge University has shown that up to 68 per cent of compulsive shoppers suffer from an affective disorder such as depression or anxiety. Experts recommend that those afflicted seek the help of a mental health professional.
For the occasional impulse shoppers out there, the next time you’re tempted, ask yourself: is it me or the dopamine talking?
It was the 14th time I hovered my thumb over the empty space where my instagram app used to be, when I realized that my social media addiction was more invasive than I thought.
As I sat on the bus that Monday morning, I felt anxious, bored and fidgety – a recipe that I knew could only be cured by scrolling through my ex-best friend’s homecoming pictures.
I’m weak. Sure enough, I re-downloaded the app on the bus. I did this so I could receive the hit of dopamine that comes with looking at pictures of humans I barely know, getting likes, comments, validation and all that fun stuff we do on our mobile devices. Dare I sit with my own thoughts and self regulate my inner dialogue for 20 minutes straight without distraction?
I often feel like I have little-to-no control over my experience with my technological devices. We have allowed it to be normal for our minds to be constantly interrupted with notifications, messages and funny dog memes.
I wish it was as easy as deleting the apps, but social media and phone usage goes deeper than that. So here I am, still grappling with how to exist in an overcrowded, oversharing world of communication – and I’m assuming you are too.
Here’s the thing: I find researching phone addictions quite frustrating. Often times article headlines will be along the lines of, “Six easy ways to get off and stay off your phone!” or “Three Simple tools to curb your phone addiction!” or even, “I got rid of my phone and my life has never been the same!”
I just don’t buy it. I feel like my phone addiction can’t be fixed with “Seven great tips” because this problem goes beyond life hacks. Similar to false weight loss diets that tell you to drink green juice and rub kale on your temples, these quick fixes are ridiculous. We need to learn more about the psychology behind why we depend on our phones, how the companies make money and how to change our philosophy.
Cal Newport, an associate professor at Georgetown University in Washington, and writer of the book Digital Minimalism, has been researching this epidemic extensively over the past few years and providing practice and frameworks to bring balance to people’s lives.
The movement Digital Minimalism is about living deliberately. Newport says when integrating new technology into your life, one must weigh their costs and benefits. One of the major costs of modern technology is solitude deprivation.
“A state in which you spend close to zero time alone with your own thoughts and free from input from other minds.”
Newport explains that having time alone creates opportunities for problem solving, self regulating, focusing, de-stressing and getting creative. Our discomfort with boredom is an epidemic, and our brains were not built for this constant stimulation. This has caused a mental health crisis. The ubiquitous nature of our cell phone use has been increasingly linked to the rise in anxiety and depression, especially in young people born after 1995.
Now is the part where I would give you a list of strategies to help you with this addiction. But alas, that would be hypocritical.
Instead, we need to educate ourselves on this overpowering issue of addiction and make significant lifestyle changes. Reading books like Newports’, researching, sharing your anxieties with peers and demanding more regulations from Facebook, Google and the powers that be are a few first steps.
Newport writes, “it’s easy to be seduced by the small amount of profit offered by the latest app or service, but then forget its cost in terms of the most important resource we possess: the minutes of our life.”
The most valuable commodity in our economy is your attention – so I hope I have it.
While one hand is holding a phone, the other is distractedly tapping on the computer keyboard – and perhaps the television is on in the background. This scene is one that we have now become obliviously acclimated to. Screens are everywhere. How often do we truly stop to recognize the impact they have on our mental health?
A recent study published in the Journal of Medical Internet Research, led by neuroscientist Najmeh Khalili-Mahani, is taking a different approach in trying to understand the relationship between screen time and stress. Most studies previously conducted look at the effects of screen time with a focus on online gaming and gambling, TV, or internet addiction. The relationship to specific types of mental disorders, such as that between depression and social networking, has become a common conversation. Khalili-Mahani’s study uses a holistic approach to analyze the interrelation between different technologies used by the same person.
“It’s a post-modern study, the relation between everything, as opposed to cause and effect between one and the other,” said Khalili-Mahani, who is also an affiliate assistant professor in the Department of Design and Computation Arts at Concordia. “We wanted to understand how the same person is using television and a smartphone. We are showing these interrelations between these technologies and this is allowing us to somehow zoom in on devices or on usages that are most likely to be associated with mental health or physical difficulties.”
The results reveal that all the different aspects of stress, such as financial or relationship difficulties, seem to be higher in individuals also suffering from screen addiction.
Moreover, the study shows that age and gender are key factors. Unsurprisingly, the effect on adults using social networks is not as significant as the younger generations or even women, said Khalili-Mahani.
“Everybody uses technology for finding information or working,” said Khalili-Mahani. “About 30 per cent of the population seems to be addicted to screens, in the sense that they are spending more than 8 hours of their daily time on the internet. Twenty per cent are also stressed and it’s those individuals who are both screen-addicted and stressed that have a significantly higher level of emotional stress.”
The study looks into individuals who already struggled with anxiety – whether emotionally or physically – and their relationship with these screens for various activities, such as relaxing, entertaining, and social networking. Computers, televisions, smartphones, all screens may serve as a coping mechanism for people who already suffer or are actively developing mental health disorders; and this is what needs to be unpacked, according to Khalili-Mahani.
As mental health is still a considerably social taboo topic, people do not necessarily associate the simple use of screens for consuming news, or work-related activities, with screen addiction. Khalili-Mahani pointed out the fact that there is a sense of social guilt when it comes to using technology, which arguably impedes the conversation surrounding screen addiction and stress. Yet, everyone is using technology, one way or another. According to Statistics Canada, the percentage of the population [using technology] is above 90 per cent in most provinces, no matter what category of addiction or stress groups they fit into.
Paradoxically, the goal of the research is not to find a solution to withdraw screen-addicted individuals from technology, but rather to develop information and communication technology, using screens for health care prevention. This could be quite a controversial approach, as some social movements are calling for technology’s total disengagement, such as quitting Facebook. Indeed, the abrupt rise of technology confronts us with a lack of comprehension, which can lead to demonization and even disdain. The more stressed or anxious someone is feeling, the greater the opportunity for escaping reality via the internet.
But finding a solution within the problem makes sense. Individuals suffering from both screen-addiction and intense levels of stress could find a familiar comfort as they are undeniably more drawn to these technologies, argued Khalili-Mahani. Using screen technologies to reach out to highly-stressed individuals and help with mental health diseases, such as depression or suicidal tendencies, are still under development. Nonetheless, it is a great step towards positively adapting rather than passively losing our inner personal battles with technology.
When I was a kid, I was told not to do drugs and the conversation ended there. If the “war on drugs” has taught us anything, it is that eliminating all drugs and forcing drug use into a specific box is both impossible and a drastic oversimplification. The rhetoric surrounding drug use currently leads to an unproductive and isolating conversation – a conversation missing one key player: drug users.
As reporters, storytellers and the ‘watchdogs of society’ we have failed time and time again at reporting on drug use. We reach out to medical professionals and policymakers, but there is a hole in this story. We wouldn’t report on someone’s art without reaching out to the artist or cover a house fire without speaking with homeowners, so why do we report on drugs without going to the source?
Harm Reduction Practitioner, Coordinator, Researcher and drug user, with the pseudonym A.C. Abbot, explains how media is missing the mark.
“The media basically doesn’t think of drug users as having opinions or expertise,” Abbot told The Concordian. They explained that we exist in a society where drug users are seen as “crazy” and “out of control.”
“The fact that drug users are denied authority and legitimacy when literally writing about drug use and drug users is telling,” added Abbot.
Journalists are feeding the biased narrative that authorities have painted for us. The media needs to approach the drug topic in a way that depicts the misconceptions of drug laws.
“Our system of drug laws is not based on scientific information about drugs,” Maia Szalavitz said, a writer from The Columbia Journalism Review. Jay Levy, the Deputy Director of the International Network of People Who Use Drugs (INPUD), explained that drug users are still being criminalized, without evidence that this attitude is in any way a productive one. Levy added that even though there are risks when using drugs, the main harm comes from laws and policies.
The judicial system, “along with their justificatory social construction and stigmas,” he continued, “are responsible for driving and worsening many of these avoidable harms.”
Portugal is often used as an example when talking about drug use and policy. The government decriminalised all drugs in 2001 and, according to the Guardian, “HIV infection plummeted from an all-time high in 2000 of 104.2 new cases per million to 4.2 cases per million in 2015.”
Although the change in law ignited a more productive conversation, it did not exist in a vacuum. Susana Ferreira, a Portuguese-Canadian freelance writer, explained that this recovery was more complex than just a change in the law.
“In many ways, the law was merely a reflection of transformations that are already happening in clinics, in pharmacies and around the kitchen tables across the country,” Ferreira wrote in a Guardian article in 2017.
A.C. Abbot thinks Portugal needs to go farther.
“It’s better to be stuck in a doctor’s office than to be stuck in a jail cell,” said Abbot, but then also explained that it’s important to be aware of the imperfect nature of medical care. Abbot said we must recognize that this environment can be a controlling one and does not always advocate for people’s autonomy. “The barriers are not only everywhere and holistic, but interweave and pulse with every other kind of prejudice.”
Although the world should be looking to Portugal in terms of drug laws, it’s crucial to continue to investigate the complexity of the situation.
“The questions aren’t just to transition from criminalization to medicalization, but it is to transition from stigmatization and problematization to autonomy,” said Abbot.
As a product of our society, I am guilty of stigmatizing drug users and drug addicts. I need to continue to push back against this stigma. This conversation leads to dehumanization and unfair treatment surrounding drug users and addicts. We must stop absorbing information at face value and learn more about the ethical discrepancies of the law. We must lean in and listen to harm reduction experts, drug users and others who are actively involved and affected by the drug stigma. We must let them lead the conversation.
Group will advise union, administration on recovery services for students
The Concordia Student Union (CSU) is launching its first addiction treatment, prevention, and recovery task force.
The CSU addiction task force is composed of five students whose mandate is to implement new addiction-harm reducing initiatives on Concordia’s campus.
The task force will be funded by the student life initiative budget, which the student life coordinator holds in order to implement any initiative for student life, including the upcoming Rapid HIV Testing Clinic.
“Addiction impacts students in a lot of different ways; it impacts their academics, it impacts their involvement in student life on campus,” said Michele Sandiford, the CSU student life coordinator and member of the task force. “We think that it is important to give them a space where they can thrive in school and thrive in the community.”
This issue is particularly important to Sandiford, who has been in recovery for two years. When she was elected as a CSU executive, she made this project part of her mandate. She said this year’s executive team has been interested in supporting mental health issues, giving her the necessary support to achieve her goal.
“For now, we really are just a body that makes recommendations to the CSU and the university, and we’re trying to implement some sort of resources or programing,” said Sandiford. “It’s about establishing recommendations for what might work for students.”
At the moment, the CSU addiction task force is a pilot project in development, while they determine what is already available to students on campus and what they might need in the future. While the launch date of the project is still unknown, the team will continue to discuss its primary focus during their weekly meetings. They also started looking into ways to promote their cause.
“We’re looking at space, we’re looking at resources, accommodations that can be made for students, and ways that we can support them,” Sandiford said. “It might be something like peer support or better access to resources.”
The team of five, including Sandiford, whose other members have not yet been revealed, is composed of students that have backgrounds in addiction recovery or have specific interest in harm-reducing or addiction treatment.
In order to maximize the task force’s impact on students in need, the group “[goes] over research, what’s already available for students, what can be made available, and from the personal experience of the members of the committee or task force,” Sandiford said. “If [students] have specific ideas for things that they might need, we’re happy to have that information brought to us,” she added.
Sandiford hopes the team will be able to bring the right help to Concordia students. She also hopes to offer students easy access to the proper assistance that many of the team’s members had a chance to get or are still going through.
Photo by Mia Anhoury.
A previous version of this article included the sentence “The Concordia Student Union (CSU) is launching its first addiction treatment, prevention, and recovery centre.” The sentence now reads: “The Concordia Student Union (CSU) is launching its first addiction treatment, prevention, and recovery task force.” In addition, the sentence “Since the task force is not fully operating yet, Sandiford advised students needing help with addiction to seek counselling for the moment,” has been removed to ensure clarity and accuracy. The Concordian regrets the errors.
How student addictions are influencing academic successes at universities
In 1929, American doctor, Gordon Alles, changed modern medicine and academia forever. Dr. Alles, a researcher for pharmaceutical giant Eli Lilly, on a mission for an allergy cure, had a colleague inject 50 mg of a chemical compound into the doctor’s arm in an attempt to test his remedy. Within minutes, Alles’s nose had cleared and amphetamine took the world by storm.
Alles noted an increased heart rate and as he wrote, “a feeling of well being“. He described feelings of alertness, euphoria, decreased appetite, and better working memory. Within years, amphetamine use exploded––soldiers in World War II used it, and companies marketed it under the brand Benzedrine for women in a “mild psychogenic depressive state.”
Amphetamine is a stimulant––a class of medications primarily used to treat Attention Deficit Hyperactivity Disorder (ADHD). Research studies have demonstrated stimulants improve quality of life by increasing underproduced neurotransmitters in the brain of those with the disorder. Modified forms of amphetamine, such as Adderall, Concerta and Vyvanse, can provide relief for those with ADHD and give them a life of normalcy.
Misuse of stimulants is not only detrimental to the user, but also to society––particularly in the academic and professional world. Without the supervision of a doctor, and more importantly the medicinal need; stimulant medications are addictive. Their short-term benefits can entice further abuse: less sleep is required, focus and energy are increased, and working memory improves.
In academia, stimulant abuse is an epidemic. A 2018 Yale University study found that between 25 per cent of students in Rocky Mountain colleges and 40 per cent of students in New England colleges reported stimulant drugs as one of the most commonly abused drug on campus. Research on Canadian abuse is far more limited, but a recent estimate is around six per cent.
And the problem is only getting worse; The Globe and Mailreported prescriptions have increased by over 30 per cent in the last five years. If this trend continues, the advantage between those who abuse stimulants over their au naturale peers will continue to become more pronounced and pose a serious risk to the meritocracy modern day academia is built upon.
Action must be taken or the devastating consequences will continue to grow for students and professionals to come. In order to acquire stimulants illicitly, a pill-seeking student needs two things: money and a drug dealer. As rates of stimulant abuse continue to rise, many students who otherwise would not abuse drugs may feel compelled to do so in order to compete with their pharmaceutically enhanced peers.
It’s no coincidence that amphetamine and methamphetamine vary by a single molecular group. When stimulants are taken incorrectly or in massive quantities, an unexpecting student may suffer anxiety, panic attacks and in extreme cases, heart attacks, psychosis or death. The normalization of recklessly pill popping before exams could seize bright students and enslave them to amphetamine. Those prone to addiction may develop a tolerance and potentially deadly addiction.
There are numerous potential solutions to prevent a grotesque marriage between “study drugs” and academic success. Doctors should screen patients rigorously before diagnosing ADHD and consider prescribing non-abusable alternatives like Wellbutrin. Other proposals are cognitive behavioural therapy and the development of coping mechanisms for less severe cases. When medications are necessary, the lowest effective dose should be prescribed and dispensed sparingly. This allows pharmacists to detect if a patient is potentially abusing their own medication or selling pills.
Education and healthcare are both pillars of an equitable and civilized society. Finding a balance between treating students with conditions like ADHD and protecting others from medications they don’t need is a delicate task. Multiple parties working in tandem can find a solution to this epidemic growing within our universities.
One student’s experience with drug addiction—and why the narrative must change
When I would come home from school, my mom would often tell me to walk the dog. This used to bother me because I hate even the most mundane exercise, but then something changed. In my senior year of high school, I started to walk the dog more often, sometimes without my mom even having to ask.
Unfortunately, my new love of dog-walking had a darker side; it became part of my routine for taking the painkiller Vicodin. Hydrocodone (the active ingredient in Vicodin) is a semi-synthetic opioid, similar to morphine. Morphine comes from the opium poppy, a plant used for decorations, bagel seasoning and heroin production, among other things.
After taking Vicodin and leashing up the dog, I would hike through the hills of my native Oregon. About half an hour into the walk, my worries of the day would begin to fade, and a sense of relaxation would overcome me. At that stage in my addiction, the pills did not impair me; in fact they helped me navigate my daily life with more ease and greater joy.
My affair with opioid painkillers (not to be confused with over-the-counter ibuprofen or Tylenol) started with a headache. Earlier in the school year, I had come home one day with a throbbing headache. I drank some water, and when that did not work, I took an aspirin. A few hours later, my head was still pounding. Out of desperation, I went into my mom’s purse and took one of her Vicodins.
At the time, I did not know how dangerous Vicodin is. I thought it was just a super strong Tylenol. My mom was recovering from surgery and had been prescribed the drug. Ironically, my grandmother, who had come from Los Angeles to take care of my mom, broke her collarbone on the flight up and left the hospital with her own 90-pill prescription. Both my mom and grandmother hated taking painkillers; this left an abundant supply for me.
When I took my first Vicodin, I was stage managing a school production involving 300 people. It was a terrific but stressful job; the Vicodin not only took away my headache but freed me from my worries.
A critical point is that my addiction could have been avoided if physicians had been more aware of the dangers of opioids at the time. Had that been the case, my mom and grandmother wouldn’t have been prescribed enormous quantities of opioids. Had there been safer prescribing practices in place, perhaps my addiction would never have started.
After that first pill, I did not take another one for a few days. Slowly, I began to develop excuses to use them—if my mom wasn’t going to take them, why should they go to waste?I developed a tolerance after a few weeks and started taking two pills to get high. Being high on painkillers isn’t like being high on other drugs. I could still function, attend school and go about my life, but everything just felt better. Nothing bothered me. I felt confident, and a warm sensation enveloped my body. At the time, I did not consider myself to be abusing drugs, and I was oblivious to this destructive pattern.
As time passed, I began to get careless. After months of a constant opioid buzz, I forgot what it felt like to be sober. Vicodin began to make me aggressive, and I started to yell more often at the actors and crew I managed at work. I stopped caring about everything, and my A in chemistry plunged to a dangerous C-. At home, my parents seemed none the wiser about my habit, and I took extraordinary steps to hide my pill-popping.
The gravy train came to an end when the pills ran out six months later. Taking the last pill in the bottle felt like a sacred event—the end of a relationship I believed I could handle on my own. Within hours, I had called my mom who was in Albuquerque. We got in an argument, and I blurted out that I had used all of her painkillers and needed help because I felt terrible. She started sobbing and flew home the next day.
My parents helped me access the resources and treatment I needed. Growing up, I never suffered from any serious mental health issues, but following my opioid use, I turned into a depressed, anxious mess. There were medications to treat my ailments, but they could only do so much. My first moments of sobriety were difficult as I mourned the end of my relationship with Vicodin. The drug turned the most mundane moments into extraordinary ones. Losing that perpetual excitement took months to get used to, and to this day, I miss the months I spent in artificial bliss.
No one wakes up one morning and decides they want to become addicted to drugs. Stealing drugs or causing my family heartache horrifies me. Opioids had an amazing capacity to mute my moral compass. Getting high no longer became something to relieve stress, but rather a necessity to remain functional and have the ability to experience happiness. Once this emotional shield began to fade, things that used to bother me enraged me; moments that hurt me devastated me and life felt like a mission without a goal.
In learning how to live without opioids, I had my “aha” moment. Most users are not lazy; they’re not failures or junkies—they are just like you and me. Often, they are just more sensitive or perhaps suffer from a mental illness.
Unfortunately, the stigma against those who suffer from substance abuse remains static with little to no improvement in public compassion. It took becoming addicted for me to realize it’s time we must shift our mentality and try to help instead of judge. Although I chose to tell my story anonymously, I hope a day will come when someone can write an article like this without hesitating to reveal who they are. Those who fight daily to stay sober ought to be celebrated as the warriors they are.
Rates of fentanyl contamination rise as a more potent opioid hits parts of Canada
Naomi Atkin had heard all about the opioid crisis. For the last three years, the 22-year-old volunteered with harm reduction organizations in Toronto. Among her responsibilities was attending concerts and raves to provide a safe support system to anyone who might have been experiencing a bad drug trip. However, it wasn’t until this summer when her former boyfriend died of a heroin overdose, that the epidemic took on a new meaning for her.
“I’d never been personally affected by it before and had someone actually die,” Atkin said.
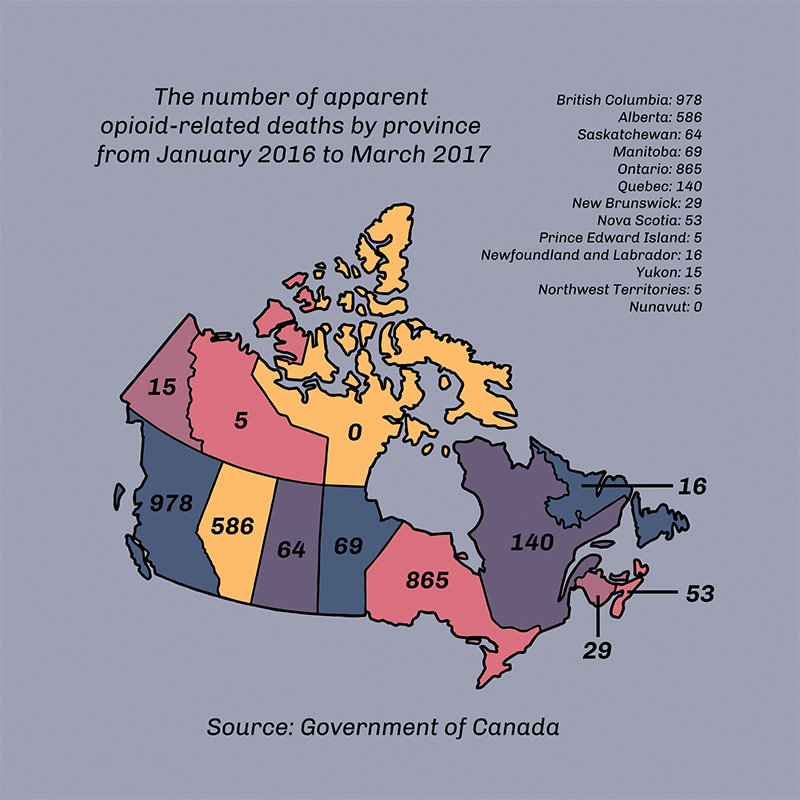
Thousands of lives have been lost in Canada because of opioid-related overdoses, spiking in the 2000s with an increase in abuse of prescription and recreational oxycodone, according to the Globe and Mail. While Oxycontin—the brand-name version of oxycodone—was removed from the pharmaceutical market in 2012, other opioids such as fentanyl and carfentanil have kept overdose rates high. Atkin’s home province of Ontario reported the second highest number of opioid-related deaths between January 2016 and March 2017, according to federal government statistics. This number, 865, was topped only by British Columbia, the province often deemed ground zero of Canada’s recent opioid epidemic. In April 2016, the province declared a public health emergency following a heightened number of fatal overdoses.
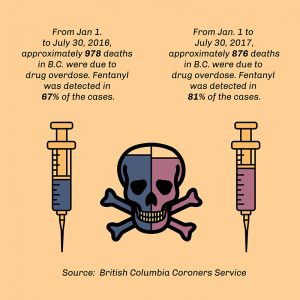
The number of opioid-related deaths in British Columbia was higher in the first six months of 2017 than it had been in that same time frame the year before. However, June saw the lowest number of deaths in 2017 in the province up to that point—a total of 111, which amounts to just under four deaths per day, according to the CBC. Despite the decrease in June, the presence of fentanyl in other illicit substances has accounted for an overall increase in drug overdoses in B.C. since 2012, according to the B.C. Coroners Service.
Fentanyl is a potent opioid pain medication typically available by prescription as a patch and about 100 times more powerful than heroin. However, it is no longer the strongest opioid being mixed with other drugs. Carfentanil—which is about 100 times more potent than fentanyl—was first detected on the streets of Vancouver in November 2016, according to the Vancouver Sun. A month later, Health Canada confirmed the opioid was found in Ontario, manufactured to resemble green Oxycontin pills. As little as 20 micrograms of carfentanil can be lethal—a little less than a pinch of salt, according to the Alberta RCMP.
In August 2016, the Calgary Police Service, the RCMP and the Canada Border Services Agency confiscated one kilogram of carfentanil at Vancouver Airport. The confiscated batch would have been enough to create 50 million deadly doses, according to the RCMP. Between September 2016 and June 2017, carfentanil was reported in Manitoba, Alberta, Ontario, Nova Scotia and in a Saskatchewan penitentiary, according to the CBC. While carfentanil has yet to be detected on the streets of Montreal, Global News reported that 209 grams of the substance were seized at the Montreal-Mirabel airport in January.
Of these two opioids, fentanyl remains the most commonly found in Canada. According to an investigation by The Globe and Mail, black market fentanyl is being manufactured in China and illegally smuggled across the Canadian border in packages weighing less than 30 grams—below the legal weight of a package border guards can open without the consent of the recipient.
Fentanyl’s low cost and high potency allows drug dealers to spend less and earn more if they cut the opioid into other drugs, most commonly heroin, to heighten their effects. Across the country, there was a 40 per cent increase in street drugs testing positive for fentanyl, Global News reported in October 2016. According to the CBC, there have been cases in Montreal of fentanyl being found in cocaine, MDMA (molly or ecstasy) and PCP, among other illicit substances.
According to Dr. Warren Steiner, who obtained his degree from McGill and has been practicing psychiatry since 1988, many of Canada’s opioid users originally got hooked on prescription painkillers.
“Doctors, as a group, over the last 10 to 20 years, have been very irresponsible in their use of prescription [opioid] painkillers, and that led to a big part of this,” said Steiner, who has been employed at the Montreal-based private rehab centre 360 DTX since its opening in 2014. Over-prescription of opioids facilitated the development of addiction among many patients, Steiner said. “Then you progress from the regular prescriptions—you start buying from the street, and you go up the ladder to the more and more potent drugs,” he added.
Included in this phenomenon is what Steiner referred to as “divergence of prescription.” In Canada, Steiner said a significant number of prescription painkillers end up in the hands of someone other than the person they were intended for. “It’s not the person they’re prescribed to who ends up taking them—they get borrowed, given away, sold on the streets,” he said. “Divergence of prescription is a big part of the drug problem, and physicians have to take responsibility—and we are. There are now courses and more and more articles and education for doctors to be much more vigilant in prescribing opiates.”
Regardless of the origins of such substance abuse, a key factor in the current opioid crisis is the frequency with which fentanyl and carfentanil end up mixed with other drugs. Based on the stories Atkin has heard, it is something she said can happen more often than most expect.
“A lot of dealers sell more than one type of drug—so someone who has a lot of cocaine might also be selling heroin or fentanyl,” she said, adding that this can lead to contamination of lesser drugs. Traces of fentanyl as little as three milligrams—while sufficient to trigger an overdose—will not be enough to evenly contaminate an entire batch of cocaine. As Atkin explained, this makes contamination less likely to show up with a drug test kit if only a portion of the batch is tested. “That’s why it’s important to be prepared,” Atkin said. “You never know when that could happen.”
Atkin recently began volunteering at a pop-up safe injection site in Moss Park in downtown Toronto because she wanted to be more involved in preventing fatal overdoses. “I think that nothing good comes to people who are using heroin because it’s just so dangerous—especially now,” she said. “I saw someone overdosing on the street just a few weeks ago.” Although she had a naloxone kit with her—the opioid overdose antidote—an ambulance arrived before she needed to use it.
“I thought about it afterwards, and even though it was such a scary experience, I would rather have been prepared for something like that, than not at all,” Atkin said. “It’s important to realize that anything can happen at any moment, and being prepared is better than the alternative.”
CLEAR SIGNS OF AN OPIOID OVERDOSE
Graphic by Zeze Le LinThe opioid epidemic flows from British Columbia, the province often deemed ground zero of Canada’s recent opioid epidemic. Graphic by Zeze Le LinGraphic by Zeze Le Lin
Cold, clammy skin. A limp body, seemingly deep in sleep. Slow breathing. A faltering or halted heartbeat. These are the symptoms of an overdose.
Imagine you and your friends are sitting around a coffee table snorting cocaine. A mid-party upper to boost your energy perhaps. You start off small, to test your tolerance. Your friend, on the other hand, snorts a larger line. Following that bump, your friend sinks back into the couch, looking dopey or at least quite out of it. They become unresponsive and look as if they’re settling into a deep sleep. They may begin snoring or choking, their fingernails or skin may turn blue, their pupils may grow small or their eyes will begin to roll back. Not only is it important to know that these are not the typical effects of cocaine use, it could also be life-saving to know that these signs are likely indicative of fentanyl or carfentanil contamination.
Death caused by an overdose can happen within minutes of ingesting the drug, although it often happens up to a few hours later after the user has fallen into a deep sleep. Nonetheless, overdoses need to be handled swiftly.
In a scenario like the one described above, call 911 immediately. Someone should check the person’s breathing—if it’s slow or shallow, inject naloxone to regulate their breathing. If naloxone is not available, administer CPR to help the person breathe until first responders arrive.
If the person’s breathing is compromised, a lack of oxygen can cause brain damage within minutes. “When you have a lot more of that substance in your blood, then other receptors are also triggered, and those receptors are decreasing the ability of the brain to breathe,” according to Dr. Sophie Gosselin, a medical toxicologist at the McGill University Health Centre. “Rather than breathing at 16 breaths per minute, some of these people breathe at eight breaths per minute, or four breaths per minute,” she said. “That’s not enough to give the body all the oxygen it needs and that’s when they go into a coma.”
If you incorrectly assess an overdose and inject naloxone, it will not harm the person, as naloxone does not induce a high—it only blocks effects of other opioids to the brain.
“A death from an opiate overdose is really someone falling asleep, losing consciousness and getting into a very deep sleep where they can’t wake up, even though they should feel the need to breath—they stop breathing and they die from that,” according to Steiner.
As Gosselin explained, when the brain does not have enough oxygen it strokes out and your heart starts to give out––sometimes the user will stop breathing all together.
“If a user experiencing an overdose has a stroke from lack of oxygen and is placed on life support, the damage has already been done,” Gosselin added. “If taken off life support, their body would not have the ability to sustain breathing alone.”
Although there are three categories of opioids—natural, synthetic and semi-synthetic—the effects these drugs have on the brain are the same. They all bind to opiate receptors in the brain. The difference is the degree in strength of each opioid.
Natural opiates, such as codeine and morphine, are commonly used to alleviate pain and accompany a variety of medical procedures. “Those activate the opiate system very mildly,” Steiner said, adding that these drugs activate only about five per cent of a person’s opiate receptors.
Stronger, semi-synthetic opioids, however, such as heroin and oxycodone, have a greater impact on receptors. “They bind very strongly to these receptors in the brain, and they really turn on the system,” Steiner said. This is what makes these substances highly addictive, but also more dangerous. “The opiate system affects the respiration and the heart, which is why people overdose and die.”
Naloxone is the medication used to counter the effects of opioids and is either injected or ingested as a nasal spray. It can reverse an overdose by blocking opiate receptors, essentially pushing the heroin or fentanyl off the receptors, Steiner explained. “[Naloxone is] something that can save many, many lives if it’s out there in the community.”
MONTREAL’S RESPONSE
The municipal government has been taking precautions over the last few months in preparation for a predicted influx of opiate overdoses. Safe injection sites were introduced at the beginning of the summer and, in September, the city announced an initiative to make naloxone more accessible.
An approximation of the amount of each drug that could induce an overdose. Photo by Alex Hutchins
Safe injection sites provide a space for users to inject drugs and, if there is a medical emergency, a healthcare worker employed at the site can attend to the person.
Two safe injection sites opened in Montreal in June: Dopamine in Hochelaga-Maisonneuve and Cactus in downtown Montreal. “For us, it has been a nine-year battle to open this site in our facility,” said Martin Pagé, the director of Dopamine. Pagé said another safe injection site is set to open in the Centre-Sud neighbourhood this fall. Once all three sites are open to the public, they are estimated to provide service for a total of 200 to 300 drug injections per day, according to Montreal Gazette.
After the centres close for the day—Dopamine closes at 1 a.m. and Cactus at 4 a.m.—a van drives around Montreal offering a mobile safe injection space. The service is called Spectre de Rue.
Safe injection sites exist in Vancouver, with plans to open others in Surrey and Victoria have been approved by the federal government. Ottawa opened its first safe injection site on Sept. 26 and Toronto currently has a pop-up site in Moss Park.
When asked if safe injection sites would encourage drug use or not, Steiner said, “People are going to use drugs and they’re going to use them badly, but you try to protect them. You can’t just say because someone’s a drug user, they deserve to die.”
On Sept. 5, Mayor Denis Coderre announced a pilot project to supply police officers and firefighters in certain boroughs with naloxone kits and training to use the antidote, according to the CBC.
Access to naloxone has been scarce in Montreal, as only four pharmacies in the city carry the antidote, according to the National Observer. Additionally, proper training on how to administer naloxone has been limited to first responders, community workers and staff at the city’s safe injection sites.
“It is an epidemic in B.C. and it’s an epidemic in Toronto and the states,” Steiner said. “I wouldn’t call it an epidemic [in Montreal], but it’s certainly a public health crisis, which we don’t want to become an epidemic.”
Safe injection sites provide the community with greater access to naloxone. However, some, like Pagé, believe there needs to be greater access outside of these sites.
Pagé said he believes naloxone kits should be distributed in Montreal. “We administer at the moment, but we do not give the kit,” Pagé said. “[Police and firefighters] should have had [naloxone] a long time ago. For us, the authorities are a bit late.”
“It’s going to come east,” he said, referring fentanyl and carfentanil. “There was no reason to think that [Eastern Canada] should be spared from this crisis.”