Saving lives and breaking down stigmas with public education
“I’m here today because there isn’t a very effective public education program,” said Richard Davy, a first-year social work student at McGill, after wrapping up the first in a series of naloxone training sessions he’s holding in November. To Davy’s delight, his first presentation on Nov. 7, which amassed an assorted crowd of students, community members and TV news crews, was a success. “People aren’t aware of this, even though we’ve known about naloxone for what seems like forever,” he added.
Naloxone, also known by its brand name Narcan, is the substance used to reverse an opioid overdose. Once administered, either nasally or through muscular injection, the naloxone blocks opioid receptors in the brain and temporarily alleviates some of the life-threatening effects of opioids. In cases of accidental overdose, it is often family, friends or bystanders who are tasked to recognize and treat an overdose, so the naloxone kits are designed to be easy-to-use for non-medical professionals.
Naloxone is also fairly easy to access; in 2017, the Quebec government began offering free naloxone kits in Quebec pharmacies to anyone 14 or older. The decision was made in reaction to the rising opioid-related hospitalization rates across Canada over the past decade. According to former Quebec Health Minister Gaétan Barrette, this was also part of a comprehensive strategy to address the public health emergency in the province that was declared after a spike in fentanyl overdoses in the summer of 2017.
Despite removing significant barriers to harm-reduction tools, the provincial government’s comprehensive strategy seems to be missing a key piece: public education. There remains a widespread lack of practical education that could equip community members with the skills and confidence required to capitalize on these resources. A 2017 opioid awareness survey by Statistics Canada found that only seven per cent of Canadians know how to both obtain and administer naloxone. Less than 30 per cent of respondents agreed that they would be able to recognize the signs of an opioid overdose.
Richard Davy, a first year social work student at McGill, held a series of naloxone training sessions throughout November. Photo by Mackenzie Lad.
Grassroots community organizations have long been doing the harm-reduction work the provincial government has only recently began to adopt in principle and practice. In 2013, Méta d’Âme, a Montreal-based “self-help organization ‘by and for’ people who depend on opioids,” created Prévenir et Réduire les Overdoses Former et Accéder à la Naloxone (PROFAN), a project focused on reducing opioid-related deaths through harm-reduction tactics, mainly the use of and access to naloxone.
PROFAN is among many longstanding independent initiatives offering informal overdose 101 education and, despite consistent action on a community level, there has yet to be a government-subsidized education program that offers the same hands-on experience.
“[Naloxone training] should be part of our repertoire of first aid. We should have an epipen in our first aid kit; we should have a naloxone kit in our first aid kit,” said Davy. “And again, that begins with education. That begins with the government getting behind it, with schools getting behind it, so we can start to raise awareness.”
Those aged 15 to 24 are within the demographic with the fastest growing rate of hospitalization for opioid poisoning according to the Canadian Institute for Health Information (CIHI). Yet youth and young adults are not formally presented with this information in an educational setting, nor are they given any collective incentive to seek it out. “If youth are going to [use substances/drugs], and they are, we need to at least give them harm-reduction tools,” said Davy. Seeing both the need for and lack of practical education at his university, Davy stepped in.
The training session not only includes step-by-step instructions of how to detect signs of an opioid overdose and how to respond using naloxone, Davy deliberately contextualized the issue to present a more comprehensive, human view of drug use and addiction. “As social workers, we’re really encouraged to look at things through a holistic lens, including the more invisible stigmas and oppressions, and I think it makes it much easier to have that deep sense of compassion for people,” said Davy. “I see the pain. I have my own history of trauma, and I connect with that when I see it in other people.”
“The absence of public education encourages more stigma and discrimination, which discourages treatment and access to treatment,” said Yamin Weiss, a fellow McGill social work student invited by Davy to share his lived experience with drug addiction and recovery. “Public opinion is huge to people internalizing a problem of addiction. A lot of people don’t seek help because they’re so stigmatized.”
Each participant left Davy’s training session with a fully-stocked naloxone kit and a new set of practical skills. Photo by Mackenzie Lad.
Naloxone may be the antidote to opioid overdose, but, according to Weiss, it will take much more to solve the underlying structural issues. “Drug addiction and recovery is something for the public to be concerned about and to care about,” said Weiss. “And public acceptance can only happen through public awareness, which is why we have Naloxone training like today.”
In its federal opioid awareness campaign, the Canadian government has broadly recognized social and structural stigma as being a pervasive force impacting the quality of and access to care for people with problematic drug use. Under the bolded “How You Can Help” heading of the government website, it is suggested that we, as Canadians, “can learn about substance use disorder and educate ourselves about the medical condition.” An auspicious idea, yet rendered ineffective without corresponding educational opportunities provided on a broad scale.
Each participant left Davy’s training session with a fully-stocked naloxone kit, a new set of practical skills, and a more nuanced view of an issue that may have seemed insurmountable from the outset. “One of my intentions with this today was to take away a little bit of the fear. Take away some of that fear and now we’re progressing” said Davy.
Davy will hold a Naloxone 101 workshop at Concordia (CSU Offices H-711) on Thursday, Nov. 22. Admission is free, but due to overwhelming demand, participants are encouraged to register beforehand via Facebook to secure a spot.
Rates of fentanyl contamination rise as a more potent opioid hits parts of Canada
Naomi Atkin had heard all about the opioid crisis. For the last three years, the 22-year-old volunteered with harm reduction organizations in Toronto. Among her responsibilities was attending concerts and raves to provide a safe support system to anyone who might have been experiencing a bad drug trip. However, it wasn’t until this summer when her former boyfriend died of a heroin overdose, that the epidemic took on a new meaning for her.
“I’d never been personally affected by it before and had someone actually die,” Atkin said.
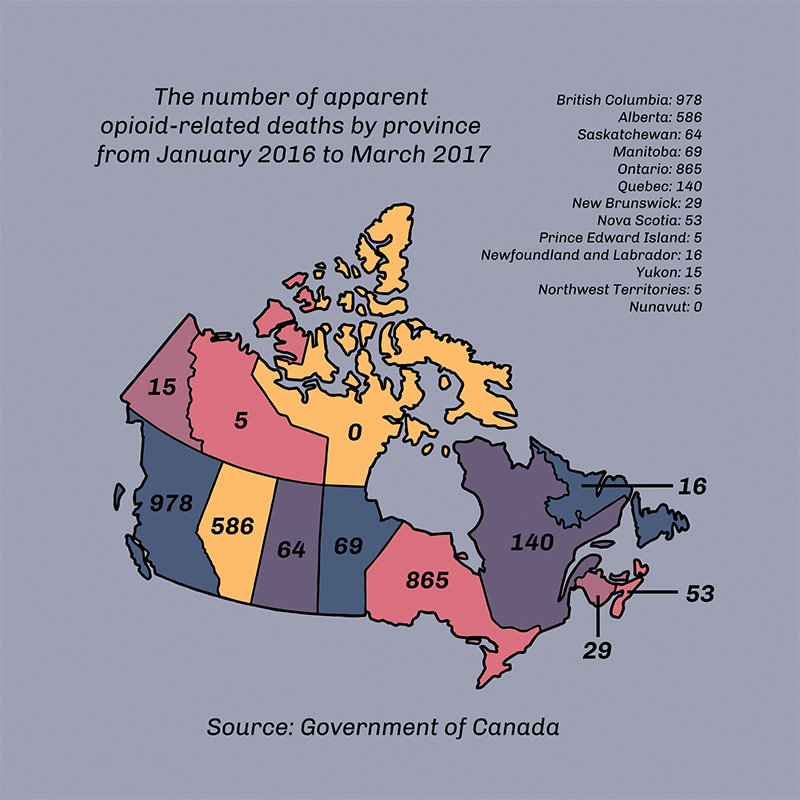
Thousands of lives have been lost in Canada because of opioid-related overdoses, spiking in the 2000s with an increase in abuse of prescription and recreational oxycodone, according to the Globe and Mail. While Oxycontin—the brand-name version of oxycodone—was removed from the pharmaceutical market in 2012, other opioids such as fentanyl and carfentanil have kept overdose rates high. Atkin’s home province of Ontario reported the second highest number of opioid-related deaths between January 2016 and March 2017, according to federal government statistics. This number, 865, was topped only by British Columbia, the province often deemed ground zero of Canada’s recent opioid epidemic. In April 2016, the province declared a public health emergency following a heightened number of fatal overdoses.
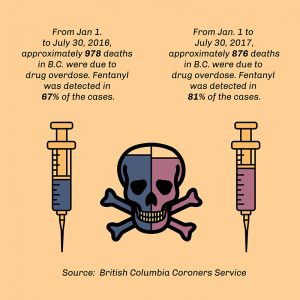
The number of opioid-related deaths in British Columbia was higher in the first six months of 2017 than it had been in that same time frame the year before. However, June saw the lowest number of deaths in 2017 in the province up to that point—a total of 111, which amounts to just under four deaths per day, according to the CBC. Despite the decrease in June, the presence of fentanyl in other illicit substances has accounted for an overall increase in drug overdoses in B.C. since 2012, according to the B.C. Coroners Service.
Fentanyl is a potent opioid pain medication typically available by prescription as a patch and about 100 times more powerful than heroin. However, it is no longer the strongest opioid being mixed with other drugs. Carfentanil—which is about 100 times more potent than fentanyl—was first detected on the streets of Vancouver in November 2016, according to the Vancouver Sun. A month later, Health Canada confirmed the opioid was found in Ontario, manufactured to resemble green Oxycontin pills. As little as 20 micrograms of carfentanil can be lethal—a little less than a pinch of salt, according to the Alberta RCMP.
In August 2016, the Calgary Police Service, the RCMP and the Canada Border Services Agency confiscated one kilogram of carfentanil at Vancouver Airport. The confiscated batch would have been enough to create 50 million deadly doses, according to the RCMP. Between September 2016 and June 2017, carfentanil was reported in Manitoba, Alberta, Ontario, Nova Scotia and in a Saskatchewan penitentiary, according to the CBC. While carfentanil has yet to be detected on the streets of Montreal, Global News reported that 209 grams of the substance were seized at the Montreal-Mirabel airport in January.
Of these two opioids, fentanyl remains the most commonly found in Canada. According to an investigation by The Globe and Mail, black market fentanyl is being manufactured in China and illegally smuggled across the Canadian border in packages weighing less than 30 grams—below the legal weight of a package border guards can open without the consent of the recipient.
Fentanyl’s low cost and high potency allows drug dealers to spend less and earn more if they cut the opioid into other drugs, most commonly heroin, to heighten their effects. Across the country, there was a 40 per cent increase in street drugs testing positive for fentanyl, Global News reported in October 2016. According to the CBC, there have been cases in Montreal of fentanyl being found in cocaine, MDMA (molly or ecstasy) and PCP, among other illicit substances.
According to Dr. Warren Steiner, who obtained his degree from McGill and has been practicing psychiatry since 1988, many of Canada’s opioid users originally got hooked on prescription painkillers.
“Doctors, as a group, over the last 10 to 20 years, have been very irresponsible in their use of prescription [opioid] painkillers, and that led to a big part of this,” said Steiner, who has been employed at the Montreal-based private rehab centre 360 DTX since its opening in 2014. Over-prescription of opioids facilitated the development of addiction among many patients, Steiner said. “Then you progress from the regular prescriptions—you start buying from the street, and you go up the ladder to the more and more potent drugs,” he added.
Included in this phenomenon is what Steiner referred to as “divergence of prescription.” In Canada, Steiner said a significant number of prescription painkillers end up in the hands of someone other than the person they were intended for. “It’s not the person they’re prescribed to who ends up taking them—they get borrowed, given away, sold on the streets,” he said. “Divergence of prescription is a big part of the drug problem, and physicians have to take responsibility—and we are. There are now courses and more and more articles and education for doctors to be much more vigilant in prescribing opiates.”
Regardless of the origins of such substance abuse, a key factor in the current opioid crisis is the frequency with which fentanyl and carfentanil end up mixed with other drugs. Based on the stories Atkin has heard, it is something she said can happen more often than most expect.
“A lot of dealers sell more than one type of drug—so someone who has a lot of cocaine might also be selling heroin or fentanyl,” she said, adding that this can lead to contamination of lesser drugs. Traces of fentanyl as little as three milligrams—while sufficient to trigger an overdose—will not be enough to evenly contaminate an entire batch of cocaine. As Atkin explained, this makes contamination less likely to show up with a drug test kit if only a portion of the batch is tested. “That’s why it’s important to be prepared,” Atkin said. “You never know when that could happen.”
Atkin recently began volunteering at a pop-up safe injection site in Moss Park in downtown Toronto because she wanted to be more involved in preventing fatal overdoses. “I think that nothing good comes to people who are using heroin because it’s just so dangerous—especially now,” she said. “I saw someone overdosing on the street just a few weeks ago.” Although she had a naloxone kit with her—the opioid overdose antidote—an ambulance arrived before she needed to use it.
“I thought about it afterwards, and even though it was such a scary experience, I would rather have been prepared for something like that, than not at all,” Atkin said. “It’s important to realize that anything can happen at any moment, and being prepared is better than the alternative.”
CLEAR SIGNS OF AN OPIOID OVERDOSE
Graphic by Zeze Le LinThe opioid epidemic flows from British Columbia, the province often deemed ground zero of Canada’s recent opioid epidemic. Graphic by Zeze Le LinGraphic by Zeze Le Lin
Cold, clammy skin. A limp body, seemingly deep in sleep. Slow breathing. A faltering or halted heartbeat. These are the symptoms of an overdose.
Imagine you and your friends are sitting around a coffee table snorting cocaine. A mid-party upper to boost your energy perhaps. You start off small, to test your tolerance. Your friend, on the other hand, snorts a larger line. Following that bump, your friend sinks back into the couch, looking dopey or at least quite out of it. They become unresponsive and look as if they’re settling into a deep sleep. They may begin snoring or choking, their fingernails or skin may turn blue, their pupils may grow small or their eyes will begin to roll back. Not only is it important to know that these are not the typical effects of cocaine use, it could also be life-saving to know that these signs are likely indicative of fentanyl or carfentanil contamination.
Death caused by an overdose can happen within minutes of ingesting the drug, although it often happens up to a few hours later after the user has fallen into a deep sleep. Nonetheless, overdoses need to be handled swiftly.
In a scenario like the one described above, call 911 immediately. Someone should check the person’s breathing—if it’s slow or shallow, inject naloxone to regulate their breathing. If naloxone is not available, administer CPR to help the person breathe until first responders arrive.
If the person’s breathing is compromised, a lack of oxygen can cause brain damage within minutes. “When you have a lot more of that substance in your blood, then other receptors are also triggered, and those receptors are decreasing the ability of the brain to breathe,” according to Dr. Sophie Gosselin, a medical toxicologist at the McGill University Health Centre. “Rather than breathing at 16 breaths per minute, some of these people breathe at eight breaths per minute, or four breaths per minute,” she said. “That’s not enough to give the body all the oxygen it needs and that’s when they go into a coma.”
If you incorrectly assess an overdose and inject naloxone, it will not harm the person, as naloxone does not induce a high—it only blocks effects of other opioids to the brain.
“A death from an opiate overdose is really someone falling asleep, losing consciousness and getting into a very deep sleep where they can’t wake up, even though they should feel the need to breath—they stop breathing and they die from that,” according to Steiner.
As Gosselin explained, when the brain does not have enough oxygen it strokes out and your heart starts to give out––sometimes the user will stop breathing all together.
“If a user experiencing an overdose has a stroke from lack of oxygen and is placed on life support, the damage has already been done,” Gosselin added. “If taken off life support, their body would not have the ability to sustain breathing alone.”
Although there are three categories of opioids—natural, synthetic and semi-synthetic—the effects these drugs have on the brain are the same. They all bind to opiate receptors in the brain. The difference is the degree in strength of each opioid.
Natural opiates, such as codeine and morphine, are commonly used to alleviate pain and accompany a variety of medical procedures. “Those activate the opiate system very mildly,” Steiner said, adding that these drugs activate only about five per cent of a person’s opiate receptors.
Stronger, semi-synthetic opioids, however, such as heroin and oxycodone, have a greater impact on receptors. “They bind very strongly to these receptors in the brain, and they really turn on the system,” Steiner said. This is what makes these substances highly addictive, but also more dangerous. “The opiate system affects the respiration and the heart, which is why people overdose and die.”
Naloxone is the medication used to counter the effects of opioids and is either injected or ingested as a nasal spray. It can reverse an overdose by blocking opiate receptors, essentially pushing the heroin or fentanyl off the receptors, Steiner explained. “[Naloxone is] something that can save many, many lives if it’s out there in the community.”
MONTREAL’S RESPONSE
The municipal government has been taking precautions over the last few months in preparation for a predicted influx of opiate overdoses. Safe injection sites were introduced at the beginning of the summer and, in September, the city announced an initiative to make naloxone more accessible.
An approximation of the amount of each drug that could induce an overdose. Photo by Alex Hutchins
Safe injection sites provide a space for users to inject drugs and, if there is a medical emergency, a healthcare worker employed at the site can attend to the person.
Two safe injection sites opened in Montreal in June: Dopamine in Hochelaga-Maisonneuve and Cactus in downtown Montreal. “For us, it has been a nine-year battle to open this site in our facility,” said Martin Pagé, the director of Dopamine. Pagé said another safe injection site is set to open in the Centre-Sud neighbourhood this fall. Once all three sites are open to the public, they are estimated to provide service for a total of 200 to 300 drug injections per day, according to Montreal Gazette.
After the centres close for the day—Dopamine closes at 1 a.m. and Cactus at 4 a.m.—a van drives around Montreal offering a mobile safe injection space. The service is called Spectre de Rue.
Safe injection sites exist in Vancouver, with plans to open others in Surrey and Victoria have been approved by the federal government. Ottawa opened its first safe injection site on Sept. 26 and Toronto currently has a pop-up site in Moss Park.
When asked if safe injection sites would encourage drug use or not, Steiner said, “People are going to use drugs and they’re going to use them badly, but you try to protect them. You can’t just say because someone’s a drug user, they deserve to die.”
On Sept. 5, Mayor Denis Coderre announced a pilot project to supply police officers and firefighters in certain boroughs with naloxone kits and training to use the antidote, according to the CBC.
Access to naloxone has been scarce in Montreal, as only four pharmacies in the city carry the antidote, according to the National Observer. Additionally, proper training on how to administer naloxone has been limited to first responders, community workers and staff at the city’s safe injection sites.
“It is an epidemic in B.C. and it’s an epidemic in Toronto and the states,” Steiner said. “I wouldn’t call it an epidemic [in Montreal], but it’s certainly a public health crisis, which we don’t want to become an epidemic.”
Safe injection sites provide the community with greater access to naloxone. However, some, like Pagé, believe there needs to be greater access outside of these sites.
Pagé said he believes naloxone kits should be distributed in Montreal. “We administer at the moment, but we do not give the kit,” Pagé said. “[Police and firefighters] should have had [naloxone] a long time ago. For us, the authorities are a bit late.”
“It’s going to come east,” he said, referring fentanyl and carfentanil. “There was no reason to think that [Eastern Canada] should be spared from this crisis.”